Acne vulgaris
coming soon
Arthritis
Anti-Inflammatory Effect of Low-Level Laser and
Light-Emitting Diode in Zymosan-Induced Arthritis
de Morais NC, Barbosa AM, Vale ML, Villaverde AB, de Lima CJ,
Cogo JC, Zamuner SR.
Laboratory of Inflammation, Institute of Research and
Development, University of Vale do Paraíba , Sáo José dos
Campos, Brazil.
Photomed Laser Surg. 2009 Sep 25. [PMID:
19780633]
Abstract Objective: The aim of this work was to investigate the
effect of low-level laser therapy (LLLT)
and light-emitting diode (LED) on
formation of edema, increase in vascular permeability, and
articular joint hyperalgesia in zymosan-induced arthritis.
Background Data: It has been suggested that low-level laser and LED
irradiation can modulate inflammatory processes.
Material and Methods: Arthritis was induced in male Wistar rats
(250-280 g) by intra-articular injection of zymosan (1 mg in 50
muL of a sterile saline solution) into one rear knee joint.
Animals were irradiated immediately, 1 h, and 2 h after zymosan
administration with a semiconductor laser (685 nm and 830 nm) and
an LED at 628 nm, with the same dose
(2.5 J/cm(2)) for laser and LED. In the
positive control group, animals were injected with the
anti-inflammatory drug dexamethasone 1 h prior to the zymosan
administration. Edema was measured by the wet/dry weight
difference of the articular tissue, the increase in vascular
permeability was assessed by the extravasation of Evans blue dye,
and joint hyperalgesia was measured using the rat knee-joint
articular incapacitation test.
Results: Irradiation with 685 nm and 830 nm laser wavelengths
significantly inhibited edema formation, vascular permeability,
and hyperalgesia. Laser irradiation, averaged over the two
wavelengths, reduced the vascular permeability by 24%, edema
formation by 23%, and articular incapacitation by 59%. Treatment
with LED (628 nm), with the same fluence
as the laser, had no effect in zymosan-induced arthritis.
Conclusion: LLLT reduces inflammatory
signs more effectively than LED
irradiation with similar irradiation times (100 sec), average
outputs (20 mW), and energy doses (2 J) in an animal model of
zymosan-induced arthritis. The anti-inflammatory effects of LLLT
appear to be a class effect, which is not wavelength specific in
the red and infrared parts of the optical spectrum.

The effect of low-level laser in knee
osteoarthritis: a double-blind, randomized, placebo-controlled
trial
Hegedus B, Viharos L, Gervain M, Gálfi M.
Physio- and Balneotherapy Center, Orosháza-Gyopáros,
Hungary. arthrodent@freemail.hu
Photomed Laser Surg. 2009 Aug;27(4):577-84. [PMID:
19530911]
INTRODUCTION: Low-level laser therapy
(LLLT) is thought to have an analgesic
effect as well as a biomodulatory effect on microcirculation. This
study was designed to examine the pain-relieving effect of LLLT
and possible microcirculatory changes measured by thermography in
patients with knee osteoarthritis (KOA).
MATERIALS AND METHODS:
Patients with mild or moderate KOA were
randomized to receive either LLLT or
placebo LLLT. Treatments were delivered
twice a week over a period of 4 wk with a diode laser (wavelength
830 nm, continuous wave, power 50 mW) in skin contact at a dose of
6 J/point. The placebo control group was treated with an
ineffective probe (power 0.5 mW) of the same appearance. Before
examinations and immediately, 2 wk, and 2 mo after completing the
therapy, thermography was performed (bilateral comparative
thermograph by AGA infrared camera);
joint flexion, circumference, and pressure sensitivity were
measured; and the visual analogue scale was recorded.
RESULTS: In the group treated with
active LLLT, a significant improvement
was found in pain (before treatment [BT]: 5.75; 2 mo after
treatment : 1.18); circumference (BT: 40.45; AT: 39.86); pressure
sensitivity (BT: 2.33; AT: 0.77); and flexion (BT: 105.83; AT:
122.94). In the placebo group, changes in joint flexion and pain
were not significant. Thermographic measurements showed at least a
0.5 degrees C increase in temperature—and thus an improvement in
circulation compared to the initial values. In the placebo group,
these changes did not occur. CONCLUSION:
Our results show that LLLT reduces pain
in KOA and improves microcirculation in
the irradiated area.
Low power laser treatment in patients with knee
osteoarthritis
Tascioglu F, Armagan O, Tabak Y, Corapci I, Oner C.
Osmangazi University, Faculty of Medicine, Department of
Physical Therapy and Rehabilitation, Eskisehir, Turkey.
fbatmaz@supronline.com
Swiss Med Wkly. 2004 May 1;134(17-18):254-8. [PMID:
15243853]
The aim of this study was to investigate the analgesic efficacy
of low power laser therapy in patients with knee osteoarthritis
(OA). The study design was randomised, placebo-controlled and
single blinded. Sixty patients with knee OA according to the
American College of Rheumatology criteria were included and
randomly assigned to three treatment groups: active laser with
dosage of 3 J/per painful point, active laser with a dosage of
1.5/J per painful point and placebo laser treatment groups. A
Gal-Al-As diode laser device was used as a source of low power
laser with a power output of 50 mW and a wavelength of 830 nm. The
patients were treated 5 times weekly with 10 treatments in all.
The clinical assessments included Western Ontario and McMaster
Universities osteoarthritis index (WOMAC)
pain, stiffness and physical function subscales. In addition, the
intensity of pain at rest and on activation was evaluated on a
visual analogue scale. Compared to baseline, at week 3 and at
month 6, no significant improvement was observed within the
groups. Similarly, no significant differences were found among the
treatment groups at any time. With the chosen laser type and dose
regimen the results that we obtained in this study, suggest that
low-level laser therapy has no effect on pain in patients with
knee OA.
Back pain
coming soon
Carpal Tunnel
Syndrome (CTS)
Carpal tunnel syndrome treated with a diode laser:
a controlled treatment of the transverse carpal ligament
Chang WD, Wu JH, Jiang JA, Yeh CY, Tsai CT.
Department of Bio-Industrial Mechatronics Engineering,
National Taiwan University, Taipei, Taiwan.
Photomed Laser Surg. 2008 Dec;26(6):551-7. [PMID:
19025407]
OBJECTIVE: The purpose of this
placebo-controlled study was to investigate the therapeutic
effects of the 830-nm diode laser on carpal tunnel syndrome (CTS).
BACKGROUND DATA:
Many articles in the literature have demonstrated that low-level
laser therapy (LLLT) may help to
alleviate various types of nerve pain, especially for CTS
treatment. We placed an 830-nm laser directly above the transverse
carpal ligament, which is between the pisiform and navicular bones
of the tested patients, to determine the therapeutic effect of LLLT.
MATERIALS AND METHODS:
Thirty-six patients with mild to moderate degree of CTS
were randomly divided into two groups. The laser group received
laser treatment (10 Hz, 50% duty cycle, 60 mW, 9.7 J/cm(2), at 830
nm), and the placebo group received sham laser treatment. Both
groups received treatment for 2 wk consisting of a 10-min laser
irradiation session each day, 5 d a week. The therapeutic effects
were assessed on symptoms and functional changes, and with nerve
conduction studies (NCS), grip strength
assessment, and with a visual analogue scale (VAS),
soon after treatment and at 2-wk follow-up.
RESULTS: Before treatment, there were no
significant differences between the two groups for all assessments
(p > 0.05). The VAS scores were
significantly lower in the laser group than the placebo group
after treatment and at follow-up (p < 0.05). After 2 wk of
treatment, no significant differences were found in grip strengths
or for symptoms and functional assessments (p > 0.05). However,
there were statistically significant differences in these
variables at 2-wk follow-up (p < 0.05). Regarding the findings
of NCS, there was no statistically
significant difference between groups after treatment and at 2-wk
follow-up.
CONCLUSIONS: LLLT
was effective in alleviating pain and symptoms, and in improving
functional ability and finger and hand strength for mild and
moderate CTS patients with no side
effects.
Ultrasound and laser therapy in the treatment of
carpal tunnel syndrome
Bakhtiary AH, Rashidy-Pour A.
Rehabilitation Faculty, Semnan Medical Sciences University,
Senman, Iran. amir822@yahoo.com.
Aust J Physiother. 2004;50(3):147-51. [PMID:
15482245]
This study was designed to compare the efficacy of ultrasound
and laser treatment for mild to moderate idiopathic carpal tunnel
syndrome. Ninety hands in 50 consecutive patients with carpal
tunnel syndrome confirmed by electromyography were allocated
randomly in two experimental groups. One group received ultrasound
therapy and the other group received low level laser therapy.
Ultrasound treatment (1 MHz, 1.0 W/cm(2), pulse 1:4, 15
min/session) and low level laser therapy (9 joules, 830 nm
infrared laser at five points) were applied to the carpal tunnel
for 15 daily treatment sessions (5 sessions/week). Measurements
were performed before and after treatment and at follow up four
weeks later, and included pain assessment by visual analogue
scale; electroneurographic measurement (motor and sensory latency,
motor and sensory action potential amplitude); and pinch and grip
strength. Improvement was significantly more pronounced in the
ultrasound group than in low level laser therapy group for motor
latency (mean difference 0.8 m/s, 95% CI 0.6 to 1.0), motor action
potential amplitude (2.0 mV, 95% CI 0.9 to 3.1), finger pinch
strength (6.7 N, 95% CI 5.0 to 8.2), and pain relief (3.1 points
on a 10-point scale, 95% CI 2.5 to 3.7). Effects were sustained in
the follow-up period. Ultrasound treatment was more effective than
laser therapy for treatment of carpal tunnel syndrome. Further
study is needed to investigate the combination therapy effects of
these treatments in carpal tunnel syndrome patients.
Noninvasive laser neurolysis in carpal tunnel
syndrome
Weintraub MI, MD, FACP
Muscle Nerve (1997) 20:1029-1031.
The peripheral nervous system is photosensitive, the scientific
rationale for this study which determines the efficacy and safety
to laser light exposure in 30 cases with CTS.
Nine joules of energy over 5 points (7-15 treatments) reversed CTS
in 77% of cases with three-fold normalization of CMAP.
A photobiologic response was seen in 80%. This unique and novel
approach is cost-effective and has a role in future management of CTS.
Treatment of repetitive use carpal tunnel syndrome
Smith CF, Vangsness CT, Anderson T & Good W (1995)
Proceedings SPIE (1995) 2395;
658-661.
A randomized, double-blind study was initiated in 1990 to
evaluate an eight-point conservative treatment program in carpal
tunnel syndrome. 160 patients were delineated with symptoms of
carpal tunnel syndrome and these patients were then divided into
two groups. Both groups were subjected to an ergonomically correct
eight-point work modification program. A counterfeit LLLT
unit was used in Group A, while an actual LLLT
unit was used in Group B. Groups A and B were statistically
significantly different in terms of return to work, conduction
study improvement, and certain range of motion.
Degenerative
disc disease
coming soon
Dental
Effects of low-level laser therapy and orthodontic
tooth movement on dental pulps in rats
Abi-Ramia LB, Sasso Stuani A, Sasso Stuani A, Sasso Stuani MB,
de Moraes Mendes A.
Angle Orthod. 2010 Jan;80(1):116-22. [PMID:
19852650]
Abstract Objectives: To describe the microscopic pulpal
reactions resulting from orthodontically induced tooth movement
associated with low-level laser therapy (LLLT)
in rats.
Materials and Methods: Forty-five young male Wistar rats were
randomly assigned to three groups. In group I (n = 20), the
maxillary right first molars were submitted to orthodontic
movement with placement of a coil spring. In group II (n = 20),
the teeth were submitted to orthodontic movement plus LLLT
at 4 seconds per point (buccal, palatal, and mesial) with a GaAlAs
diode laser source (830 nm, 100 mW, 18 J/cm(2)). Group III
(n = 5) served as a control (no orthodontic movement or LLLT).
Groups I and II were divided into four subgroups according to the
time elapsed between the start of tooth movement and sacrifice (12
hours, 24 hours, 3 days, and 7 days).
Results: Up until the 3-day period, the specimens in group I
presented a thicker odontoblastic layer, no cell-free zone of
Weil, pulp core with differentiated mesenchymal and defense cells,
and a high concentration of blood vessels. In group II, at the 12-
and 24-hour time points, the odontoblastic layer was disorganized
and the cell-free zone of Weil was absent, presenting
undifferentiated cells, intensive vascularization with congested
capillaries, and scarce defense cells in the cell-rich zone. In
groups I and II, pulpal responses to the stimuli were more intense
in the area underneath the region of application of the force or
force/laser.
Conclusions: The orthodontic-induced tooth movement and LLLT
association showed reversible hyperemia as a tissue response to
the stimulus. LLLT leads to a faster
repair of the pulpal tissue due to orthodontic movement.
The short-term effects of low-level lasers as
adjunct therapy in the treatment of periodontal inflammation
Qadri T, Miranda L, Tunér J, Gustafsson A.
Department of Periodontology, Institute of Odontology,
Karolinska Institutet, Huddinge, Sweden.
talat.qadri@mbox.lidnet.se
J Clin Periodontol. 2005 Jul;32(7):714-9. [PMID:
15966876]
OBJECTIVES: The aim of this
split-mouth, double-blind controlled clinical trial was to study
the effects of irradiation with low-level lasers as an adjunctive
treatment of inflamed gingival tissue.
MATERIALS AND METHODS:
Seventeen patients with moderate periodontitis were included.
After clinical examination, all teeth were scaled and root planed
(SRP). One week after SRP,
we took samples of gingival crevicular fluid (GCF)
and subgingival plaque. The laser therapy was started 1 week later
and continued once a week for 6 weeks. One side of the upper jaw
was treated with active laser and the other with a placebo. The
test side was treated with two low-level lasers having wavelengths
of 635 and 830 nm. The patients then underwent another clinical
examination with sampling of GCF and
plaque. The GCF samples were analysed
for elastase activity, interleukin-1beta (IL-1beta) and
metalloproteinase-8 (MMP-8). We examined
the subgingival plaque for 12 bacteria using DNA
probes.
RESULTS: The clinical variables i.e.
probing pocket depth, plaque and gingival indices were reduced
more on the laser side than on the placebo one (p<0.01). The
decrease in GCF volume was also greater
on the laser side, 0, 12 microl, than on the placebo side, 0.05
microl (p=0.01). The total amount of MMP-8
increased on the placebo side but was slightly lower on the laser
side (p=0.052). Elastase activity, IL-1beta concentration and the
microbiological analyses showed no significant differences between
the laser and placebo sides.
CONCLUSION: Additional treatment with
low-level lasers reduced periodontal gingival inflammation.
Effect of low-level laser therapy on Candida
albicans growth in patients with denture stomatitis.
Maver-Biscanin M, Mravak-Stipetic M, Jerolimov V.
Department of Prosthodontics, Clinical Hospital Centre,
Zagreb, Croatia. mirela.maver@zg.htnet.hr
Photomed Laser Surg. 2005 Jun;23(3):328-32. [PMID:
15954824]
OBJECTIVE: The purpose of our report
is to present the effect of low-level laser therapy on Candida
albicans growth and palatal inflammation in two patients with
denture stomatitis. BACKGROUND DATA:
The most common oral mucosal disorder in denture wearers is
denture stomatitis, a condition that is usually associated with
the presence of the yeast Candida albicans. Different treatment
methods have been suggested to treat this symptom, none of which
is proven to be absolutely effective.
METHODS: Two denture-wearing patients,
both with palatal inflammation diagnosed as Newton type II denture
stomatitis were treated with low-power semiconductor diode laser (BTL-2000,
Prague, Czech Republic) at different wavelengths (685 and 830 nm)
for 5 d consecutively. In both patients, palatal mucosa and
acrylic denture base were irradiated in noncontact mode (probe
distance of 0.5 cm from irradiated area) with different exposure
times-5 min (830 nm, 3.0 J/cm2, 60 mW) and 10 min (685 nm, 3.0
J/cm2, 30 mW). The effect of laser light on fungal growth in vivo
was evaluated after the final treatment using the swab method and
semiquantitative estimation of Candida albicans colonies growth on
agar plates. The severity of inflammation was evaluated using
clinical criteria.
RESULTS: After lowlevel laser treatment,
the reduction of yeast colonies on the agar plates was observed
and palatal inflammation was diminished.
CONCLUSION: LLLT
is effective in the treatment of denture stomatitis. Further
placebo controlled studies are in progress.
Laser therapy in the treatment of dentine
hypersensitivity
Ladalardo TC, Pinheiro A, Campos RA, Brugnera Júnior A, Zanin
F, Albernaz PL, Weckx LL.
Federal University of São Paulo, UNIFESP-EPM,
São Paulo, SP, Brazil. t.chris@uol.com.br
Braz Dent J. 2004;15(2):144-50. Epub 2005 Mar 11. [PMID:
15776198]
Cervical dentine hypersensitivity is the most frequent
complaint among reported odontalgias. Thus, this study evaluated
the effectiveness of two types of lasers (660 nm wavelength red,
and 830 nm wavelength infrared) as dentine desensitizers, as well
as both the immediate and late therapeutic effects in individuals
25 to 45 years of age. A total of 40 teeth with cervical exposure
were treated in 4 sessions. They were divided into 2 groups
according to treatment. A 660 nm wavelength red diode laser and an
830 nm wavelength infrared diode laser were used. Dentine
sensitivity to cold nociceptive stimulus was evaluated by means of
a pain numeric scale from zero to 10 before each treatment
session, at 15 and 30 min after irradiation, and in a follow-up
period of 15, 30 and 60 days after the end of treatment.
Significant levels of dentinal desensitization were only found in
patients ranging in age from 25 to 35 years. The 660 nm red diode
laser was more effective than the 830 nm infrared laser and a
higher level of desensitization was observed at the 15 and 30
minute post-irradiation examinations. The immediate and late
therapeutic effects of the 660 nm red diode laser were more
evident in 25-35-year-old patients compared with those of the 830
nm infrared diode laser, in terms of the different age groups.
Fibromyalgia
Efficacy of low power laser therapy in
fibromyalgia: a single-blind, placebo-controlled trial
Gür A, Karakoç M, Nas K, Cevik R, Saraç J, Demir E.
Physical Medicine and Rehabilitation, School of Medicine,
Dicle University, Diyarbakir, Turkey. alig@dicle.edu.tr
Lasers Med Sci. 2002;17(1):57-61. [PMID:
11845369]
Low energy lasers are widely used to treat a variety of
musculoskeletal conditions including fibromyalgia, despite the
lack of scientific evidence to support its efficacy. A randomised,
single-blind, placebo-controlled study was conducted to evaluate
the efficacy of low-energy laser therapy in 40 female patients
with fibromyalgia. Patients with fibromyalgia were randomly
allocated to active (Ga-As) laser or placebo laser treatment daily
for two weeks except weekends. Both the laser and placebo laser
groups were evaluated for the improvement in pain, number of
tender points, skinfold tenderness, stiffness, sleep disturbance,
fatigue, and muscular spasm. In both groups, significant
improvements were achieved in all parameters (p<0.05) except
sleep disturbance, fatigue and skinfold tenderness in the placebo
laser group (p>0.05). It was found that there was no
significant difference between the two groups with respect to all
parameters before therapy whereas a significant difference was
observed in parameters as pain, muscle spasm, morning stiffness
and tender point numbers in favour of laser group after therapy
(p<0.05). None of the participants reported any side effects.
Our study suggests that laser therapy is effective on pain, muscle
spasm, morning stiffness, and total tender point number in
fibromyalgia and suggests that this therapy method is a safe and
effective way of treatment in the cases with fibromyalgia.
Herniated discs
coming soon
Inflammation
Effects of Laser on the Synovial Fluid in the
Inflammatory Process of the Knee Joint of the Rabbit
Sandoval MC, Mattiello-Rosa SM, Soares EG, Parizotto NA.
School of Physical Therapy, Industrial University of
Santander, Bucaramanga, Columbia.
Photomed Laser Surg. 2009 Feb 2 [PMID:
19187016]
Abstract Objective: The purpose of this study was to evaluate
the effects of low-level laser (LLL)
energy on the clinical signs of inflammation and the cellular
composition of synovial fluid (SF) in the inflamed knee of the
rabbit. Background Data: There are few findings related to the
effects of LLL on SF in inflammatory
processes and there is little knowledge about the optimal
parameters for reducing joint inflammation. Materials and Methods:
Inflammation in the right knee of 36 rabbits was induced by
intracapsular injection (0.2 mL) of Terebinthina commun (Tc). The
animals were randomly assigned to three groups: acute experimental
group (AEG), chronic experimental group
(CEG), and control group (CG), which
only received Tc. Each group was divided in two subgroups of six
animals each. The AEG and CEG
groups began to receive laser treatment 2 and 5 d after the
induction of inflammation, respectively. Laser irradiation at a
wavelength of 830 nm, power output of 77 mW, and power density of
27.5 W/cm(2) was applied daily for 7 d for either 0.12 sec or 0.32
sec, resulting in doses of 3.4 J/cm(2) and 8 J/cm(2),
respectively. Body mass, joint perimeter, joint temperature, and
the morphology of the SF were analyzed. Results: There was no
statistically significant differences between groups in the body
mass, joint perimeter, and SF morphology. Conclusion: Laser
irradiation with the selected parameters produced only a few
subtle differences in the inflammatory signs and the SF. The lack
of effects may have been due to the short irradiation time.
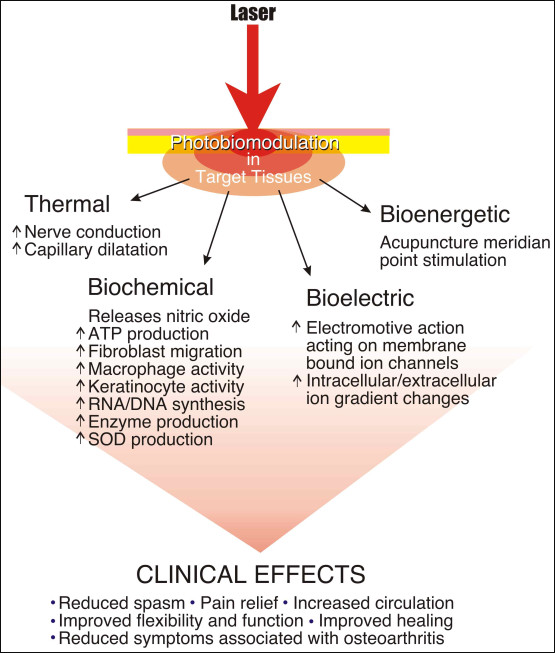
Laser-Accelerated INFLAMMATION/PAIN
REDUCTION AND HEALING
by Richard Martin, BS, CLT
Practical Pain Management, Nov/Dec 2003
Injured cells and tissues have greater affinity for LLLT
than healthy cells and tissues. LLLT in
the treatment of inflammation, pain and healing is a highly
integrated process, but the author separates those processes
categorically for identification.
Acute Inflammation Reduction(flowchart
provided in the original article) – After injury, tissues
initiate a series of biological responses and cellular membrane
reactions which manifest in a combination of edema, inflammation,
pain and functional debility. LLLT
mediates by: (1) Stabilizing cellular membranes; (2) Enhancing
molecule ATP production and synthesis;
(3) Stimulating vasodilation via increased Histamine, Nitric Oxide
and Serotonin; (4) Accelerating leukocytic activity; (5)
Increasing Prostaglandin synthesis; (6) Reducing Interleukin-1;
(7) Enhancing lymphocyte response; (8) Increasing angiogenesis;
(9) Modulation temperature; (10) Enhancing superoxide dismutase
levels; and (11) Decreasing C-reactive protein and neopterin
levels.
Pain Reduction(flowchart provided in the
original article) – Evidence justifies a conclusion that LLLT
reduces pain by combination of processes: (1) Increase in
b-Endorphins; (2) Blocked depolarization of C-fiber afferent
nerves; (3) Increased nitric oxide production; (4) Increased nerve
cell action potential; (5) Axonal sprouting and nerve cell
regeneration; (6) Decreased Bradykinin levels; (7) Increased
release of acetylcholine; and (8) Ion channel normalization.
Tissue Healing – LLLT
enhances wound healing by: (1) Enhanced leukocyte infiltration;
(2) Increased macrophage activity; (3) Increased
neovascularization; (4) Increased fibroblast proliferation; (5)
Keratinocyte proliferation; (6) Early epithelialization; (7)
Growth factor increases; (8) Enhanced cell proliferation and
differentiation, and (9) Greater healed wound tensile strength.
Joint pain
LLLT with trigger points
technique: clinical study on 243 patients
Simunovic Z
Journal of Clinical Laser Medicine and Surgery (Aug. 1996)
14(4):163-167.
Among the various methods of application techniques in LLLT
(He-Ne 632.8 nm visible red or infrared 820-830 nm continuous wave
and 904 nm pulsed emission) there are very promising “trigger
points”, i.e., myofascial zones of particular sensibility and of
highest projection of focal pain points, due to ischemic
conditions. The effect of LLT and the
results obtained after clinical treatment of >200 patients
(headaches and facial pain, skeletomuscular ailments, myogenic
neck pain, shoulder and arm pain, epicondylitis, tenosynovitis,
low back and radicular pain, Achilles tendonitis) to whom the
“trigger points” were applied were better than expected. It
was also observed that rigidity decreases, mobility is restored
(functional recovery), and spontaneous or induced pain decreases
or even disappears, by movement. LLLT
improves local microcirculation and it can also improve oxygen
supply to hypoxic cells in the treated areas and can remove
collected waste products. Normalization of the microcirculation
interrupts the “circulus vitiosus” of the origin of the pain
and its development (Melzak: muscular
tension→pain→increased tension→increased pain,
etc.). Results measured according to VAS/VRS/PTM:
in acute pain, diminished >70%; in chronic pain >60%.
Clinical effectiveness depends on correctly applied energy dose
– over/under dosage produces opposite, negative effects on
cellular metabolism. No negative effects were noted and the use of
analgesic drugs could be reduced or completely excluded. LLLT
may be used as monotherapy or as a supplement to other therapeutic
procedures for pain treatment.
Lesions
Analysis of Low-Level Laser Radiation Transmission
in Occlusive Dressings
de Jesus Guirro RR, de Oliveira Guirro EC, Martins CC, Nunes
FR.
Department of Biomechanics, Medicine and Rehabilitation of the
Locomotor System, School of Medicine of Ribeirão Preto,
University São Paulo, Brazil
Photomed Laser Surg. 2009 Oct 9. [PMID:
19817516]
Abstract Objective: The purpose of this study is to analyze the
power transmitted by low-level laser therapy (LLLT)
into occlusive dressings using different wavelengths for the
treatment of cutaneous lesions.
Background Data: LLLT has been largely
used to treat several cutaneous lesions commonly associated with
occlusive dressings to accelerate the healing process.
Materials and Methods: Radiation transmission was measured by a
digital power analyzer connected to a laser emitter with
wavelengths of 660, 830, and 904 nm and mean levels of 30, 30, 6.5
mW, respectively, previously calculated. Thirteen different
occlusive dressings were analyzed and interposed between the laser
emitter and the power analyzer sensor, with 15 measurements made
for each dressing. Statistics were provided by the analysis of
variance (ANOVA), followed by
Student’s t-test (p < 0.05).
Results: The power transmitted ranged between 98.6% and 0%,
depending on the material and wavelength. The dressings tested
were BioFill, Hydrofilm, Confeel Plus 3533, Confeel 3218, DuoDERM
Extra Thin, Hydrocoll, Micropore Nexcare, CIEX
tape, Emplasto Sábia, CombiDERM, Band-aid, Actisorb Plus, in
addition to polyvinylchloride (PVC)
film, and transmitted power higher than 40% of the incident power,
independently from the wavelength indicated for the association
with LLLT.
Conclusion: The results showed that LLLT
transmission depends on the occlusive dressing material and the
wavelength irradiated.
Effect of low level laser therapy (830 nm) with
different therapy regimes on the process of tissue repair in
partial lesion calcaneous tendon
Oliveira FS, Pinfildi CE, Parizoto NA, Liebano RE, Bossini PS,
Garcia EB, Ferreira LM.
Department of Plastic Surgery, São Paulo Federal University-UNIFESP,
São Paulo, SP 04024-900, Brazil.
Lasers Surg Med. 2009 Apr;41(4):271-6. [PMID:
19347936]
BACKGROUND AND
OBJECTIVE: Calcaneous tendon is one of
the most damaged tendons, and its healing may last from weeks to
months to be completed. In the search after speeding tendon
repair, low intensity laser therapy has shown favorable effect. To
assess the effect of low intensity laser therapy on the process of
tissue repair in calcaneous tendon after undergoing a partial
lesion.
STUDY DESIGN/MATERIALS
AND METHODS:
Experimentally controlled randomized single blind study. Sixty
male rats were used randomly and were assigned to five groups
containing 12 animals each one; 42 out of 60 underwent lesion
caused by dropping a 186 g weight over their Achilles tendon from
a 20 cm height. In Group 1 (standard control), animals did not
suffer the lesion nor underwent laser therapy; in Group 2
(control), animals suffered the lesion but did not undergo laser
therapy; in Groups 3, 4, and 5, animals suffered lesion and
underwent laser therapy for 3, 5, and 7 days, respectively.
Animals which suffered lesion were sacrificed on the 8th day after
the lesion and assessed by polarization microscopy to analyze the
degree of collagen fibers organization.
RESULTS: Both experimental and standard
control Groups presented significant values when compared with the
control Groups, and there was no significant difference when
Groups 1 and 4 were compared; the same occurred between Groups 3
and 5.
CONCLUSION: Low intensity laser therapy
was effective in the improvement of collagen fibers organization
of the calcaneous tendon after undergoing a partial lesion.
Muscle
spasms
coming soon
Neck pain
Efficacy of low-level laser therapy in the
management of neck pain: a systematic review and meta-analysis of
randomised placebo or active-treatment controlled trials
Chow RT, Johnson MI, Lopes-Martins RA, Bjordal JM.
Nerve Research Foundation, Brain and Mind Research Institute,
University of Sydney, Sydney, NSW,
Australia. robertachow@iinet.net.au
Lancet. 2009 Dec 5;374(9705):1897-908. Epub 2009 Nov 13. [PMID:
19913903]
BACKGROUND: Neck pain is a common and
costly condition for which pharmacological management has limited
evidence of efficacy and side-effects. Low-level laser therapy (LLLT)
is a relatively uncommon, non-invasive treatment for neck pain, in
which non-thermal laser irradiation is applied to sites of pain.
We did a systematic review and meta-analysis of randomised
controlled trials to assess the efficacy of LLLT
in neck pain.
METHODS: We searched computerised
databases comparing efficacy of LLLT
using any wavelength with placebo or with active control in acute
or chronic neck pain. Effect size for the primary outcome, pain
intensity, was defined as a pooled estimate of mean difference in
change in mm on 100 mm visual analogue scale.
FINDINGS: We identified 16 randomised
controlled trials including a total of 820 patients. In acute neck
pain, results of two trials showed a relative risk (RR) of 1.69
(95% CI 1.22-2.33) for pain improvement of LLLT
versus placebo. Five trials of chronic neck pain reporting
categorical data showed an RR for pain improvement of 4.05
(2.74-5.98) of LLLT. Patients in 11
trials reporting changes in visual analogue scale had pain
intensity reduced by 19.86 mm (10.04-29.68). Seven trials provided
follow-up data for 1-22 weeks after completion of treatment, with
short-term pain relief persisting in the medium term with a
reduction of 22.07 mm (17.42-26.72). Side-effects from LLLT
were mild and not different from those of placebo.
INTERPRETATION: We show that LLLT
reduces pain immediately after treatment in acute neck pain and up
to 22 weeks after completion of treatment in patients with chronic
neck pain. FUNDING: None.
Click
here to read the complete study.
-——————————————————————————————————————-
The effect of 300 mW, 830 nm laser on chronic neck
pain: a double-blind, randomized, placebo-controlled study
Chow RT, Heller GZ, Barnsley L.
Castle Hill Medical Centre, 269-271 Old Northern Road, Castle
Hill, NSW 2154, Australia.
rtchow@bigpond.net.au
Pain. 2006 Sep;124(1-2):201-10. Epub 2006 Jun 27. [PMID:
16806710]
A randomized, double-blind, placebo-controlled study of
low-level laser therapy (LLLT) in 90
subjects with chronic neck pain was conducted with the aim of
determining the efficacy of 300 mW, 830 nm laser in the management
of chronic neck pain. Subjects were randomized to receive a course
of 14 treatments over 7 weeks with either active or sham laser to
tender areas in the neck. The primary outcome measure was change
in a 10 cm Visual Analogue Scale (VAS)
for pain. Secondary outcome measures included Short-Form 36
Quality-of-Life questionnaire (SF-36), Northwick Park Neck Pain
Questionnaire (NPNQ), Neck Pain and
Disability Scale (NPAD), the McGill Pain
Questionnaire (MPQ) and Self-Assessed
Improvement (SAI) in pain measured by VAS.
Measurements were taken at baseline, at the end of 7 weeks’
treatment and 12 weeks from baseline. The mean VAS
pain scores improved by 2.7 in the treated group and worsened by
0.3 in the control group (difference 3.0, 95% CI 3.8-2.1).
Significant improvements were seen in the active group compared to
placebo for SF-36-Physical Score (SF36 PCS),
NPNQ, NPAD, MPQVAS
and SAI. The results of the SF-36 –
Mental Score (SF36 MCS) and other MPQ
component scores (afferent and sensory) did not differ
significantly between the two groups. Low-level laser therapy (LLLT),
at the parameters used in this study, was efficacious in providing
pain relief for patients with chronic neck pain over a period of 3
months.
Systematic review of the literature of low-level
laser therapy (LLLT) in the management
of neck pain
Chow RT, Barnsley L.
Castle Hill Medical Centre, Castle Hill Medical Centre,
269-271 Old Northern Road, Castle Hill, New South Wales 2154,
Australia. rtchow@bigpond.net.au
Lasers Surg Med. 2005 Jul;37(1):46-52. [PMID:
15954117]
BACKGROUND AND
OBJECTIVES: Low-level laser therapy (LLLT)
is widely used in the treatment of musculoskeletal pain. However,
there is controversy over its true efficacy. We aimed to determine
the efficacy of LLLT in the treatment of
neck pain through systematically reviewing the literature.
STUDY DESIGN/MATERIALS
AND METHODS: A
search of computerized bibliographic databases covering medicine,
physiotherapy, allied health, complementary medicine, and
biological sciences was undertaken undertaken from date of
inception until February 2004 for randomized controlled trials of LLLT
for neck pain. A comprehensive list of search terms was applied
and explicit inclusion criteria were developed a priori. Twenty
studies were identified, five of which met the inclusion criteria.
RESULTS: Significant positive effects
were reported in four of five trials in which infrared wavelengths
(lambda = 780, 810-830, 904, 1,064 nm) were used. Heterogeneity in
outcome measures, results reporting, doses, and laser parameters
precluded formal meta-analysis. Effect sizes could be calculated
for only two of the studies.
CONCLUSIONS: This review provides
limited evidence from one RCT for the
use of infrared laser for the treatment of acute neck pain (n =
71) and chronic neck pain from four RCTs (n = 202). Larger studies
are required to confirm the positive findings and determine the
most effective laser parameters, sites and modes of application.
© 2005 Wiley-Liss, Inc.
Plantar
Fasciitis
coming soon
Post-surgical
pain
Effects of Low-Level Laser Therapy on Pain and Scar
Formation after Inguinal Herniation Surgery: A Randomized
Controlled Single-Blind Study
de Paiva Carvalho RL, Alcântara PS, Kamamoto F, Cressoni MD,
Casarotto RA.
Postgraduate Program in Rehabilitation Sciences , University
of São Paulo, São Paulo, Brazil.
Photomed Laser Surg. 2009 Oct 12. [PMID:
19821701]
Abstract Objective: The aim of this study was to investigate
the efficacy of an infrared GaAlAs laser operating with a
wavelength of 830 nm in the postsurgical scarring process after
inguinal-hernia surgery. Background: Low-level laser therapy (LLLT)
has been shown to be beneficial in the tissue-repair process, as
previously demonstrated in tissue culture and animal experiments.
However, there is lack of studies on the effects of LLLT
on postsurgical scarring of incisions in humans using an infrared
830-nm GaAlAs laser. Method: Twenty-eight patients who underwent
surgery for inguinal hernias were randomly divided into an
experimental group (G1) and a control group (G2). G1 received LLLT,
with the first application performed 24 h after surgery and then
on days 3, 5, and 7. The incisions were irradiated with an 830-nm
diode laser operating with a continuous power output of 40 mW, a
spot-size aperture of 0.08 cm(2) for 26 s, energy per point of
1.04 J, and an energy density of 13 J/cm(2). Ten points per scar
were irradiated. Six months after surgery, both groups were
reevaluated using the Vancouver Scar Scale (VSS),
the Visual Analog Scale, and measurement of the scar thickness.
Results: G1 showed significantly better results in the VSS
totals (2.14 +/- 1.51) compared with G2 (4.85 +/- 1.87); in the
thickness measurements (0.11 cm) compared with G2 (0.19 cm); and
in the malleability (0.14) compared with G2 (1.07). The pain score
was also around 50% higher in G2.
Conclusion: Infra-red LLLT (830 nm)
applied after inguinal-hernia surgery was effective in preventing
the formation of keloids. In addition, LLLT
resulted in better scar appearance and quality 6 mo postsurgery.
Comparative study using 685-nm and 830-nm lasers in
the tissue repair of tenotomized tendons in the mouse
Carrinho PM, Renno AC, Koeke P, Salate AC, Parizotto NA, Vidal
BC.
Laboratory of Electro-Thermo-Phototherapy, Department of
Physiotherapy, Federal University of São Carlos, São Carlos,
Brazil.
Photomed Laser Surg. 2006 Dec;24(6):754-8. [PMID:
17199477]
OBJECTIVE: The objective of this
study was to evaluate the effects of 685- and 830-nm laser
irradiations, at different fluences on the healing process of
Achilles tendon (Tendon calcaneo) of mice after tenotomy.
BACKGROUND DATA:
Some authors have shown that low-level laser therapy (LLLT)
is able to accelerate the healing process of tendinuos tissue
after an injury, increasing fibroblast cell proliferation and
collagen synthesis. However, the mechanism by which LLLT
acts on healing process is not fully understood.
METHODS: Forty-eight male mice were
divided into six experimental groups: group A, tenomized animals,
treated with 685 nm laser, at the dosage of 3 J/cm(2); group B,
tenomized animals, treated with 685-nm laser, at the dosage of 10
J/cm(2); group C, tenomized animals, treated with 830-nm laser, at
dosage of 3 J/cm(2); group D, tenomized animals, treated with
830-nm laser, at the dosage of 10 J/cm(2); group E, injured
control (placebo treatment); and group F, non-injured standard
control. Animals were killed on day 13 post-tenotomy, and their
tendons were surgically removed for a quantitative analysis using
polarization microscopy, with the purpose of measuring collagen
fibers organization through the birefringence (optical retardation
[OR]).
RESULTS: All treated groups showed
higher values of OR when compared to injured control group. The
best organization and aggregation of the collagen bundles were
shown by the animals of group A (685 nm, 3 J/cm(2)), followed by
the animals of group C and B, and finally, the animals of group D.
CONCLUSION: All wavelengths and fluences
used in this study were efficient at accelerating the healing
process of Achilles tendon post-tenotomy, particularly after the
685-nm laser irradiation, at 3 J/cm(2). It suggests the existence
of wavelength tissue specificity and dose dependency. Further
studies are required to investigate the physiological mechanisms
responsible for the effects of laser on tendinuos repair.
Post-trauma
acute pain
THE USE
OF LASER THERAPY
AND ADDITIONAL
THERAPEUTIC MODALITIES
AFTER ARTHROSCOPY
OF THE KNEE AT
ALPINE SKI TEAM
Lilic Alen, physiotherapist; 2Kozlevcar ivec Maja, dr. med.
spec.fiz.reh.med.; 3Marcan Radoslav, dr.med., spec.ortop 1FIZIO,
Ilirska Bistrica, Slovenija, 2Iskra Medical, Ljubljana, Slovenija,
3Ortopedska bolninica Valdoltra, Slovenija.
We review different kinds of injuries in the alpine ski sport
concentrate on the injuries of the ligamentar part of the knees
and meniscs in slovenian ski team. After the description of the
injuries is a detailed presentation of the rehabilitational
procedures from the first day of the injury till the return in to
the competition arena. We explain the modalities of the
rehabilitational procedures and their influence in the tissues,
their main and side effects. Our main attention is focused on the
use of the biostimulative lasers of higher power – 1,2 W and
wavelength of 830 nm and their influence speedy recovery of the
patients and their success in later competitions.
Posterior
facet syndrome
coming soon
Sciatica
coming soon
Sprains
and strains
coming soon
Tendonitis
A systematic review with procedural assessments and
meta-analysis of low level laser therapy in lateral elbow
tendinopathy (tennis elbow)
Bjordal JM, Lopes-Martins RA, Joensen J, Couppe C, Ljunggren
AE, Stergioulas A, Johnson MI.
Institute of Physiotherapy, Faculty of Health and Social
Sciences, Bergen University College, Moellendalsvn, 6, 5009
Bergen, Norway. jmb@hib.no
BMC Musculoskelet Disord. 2008 May
29;9:75. [PMID: 18510742]
BACKGROUND: Recent reviews have
indicated that low level level laser therapy (LLLT)
is ineffective in lateral elbow tendinopathy (LET)
without assessing validity of treatment procedures and doses or
the influence of prior steroid injections.
METHODS: Systematic review with
meta-analysis, with primary outcome measures of pain relief and/or
global improvement and subgroup analyses of methodological
quality, wavelengths and treatment procedures.
RESULTS: 18 randomised
placebo-controlled trials (RCTs) were identified with 13 RCTs (730
patients) meeting the criteria for meta-analysis. 12 RCTs
satisfied half or more of the methodological criteria. Publication
bias was detected by Egger’s graphical test, which showed a
negative direction of bias. Ten of the trials included patients
with poor prognosis caused by failed steroid injections or other
treatment failures, or long symptom duration or severe baseline
pain. The weighted mean difference (WMD)
for pain relief was 10.2 mm [95% CI: 3.0 to 17.5] and the RR for
global improvement was 1.36 [1.16 to 1.60]. Trials which targeted
acupuncture points reported negative results, as did trials with
wavelengths 820, 830 and 1064 nm. In a subgroup of five trials
with 904 nm lasers and one trial with 632 nm wavelength where the
lateral elbow tendon insertions were directly irradiated, WMD
for pain relief was 17.2 mm [95% CI: 8.5 to 25.9] and 14.0 mm [95%
CI: 7.4 to 20.6] respectively, while RR for global pain
improvement was only reported for 904 nm at 1.53 [95% CI: 1.28 to
1.83]. LLLT doses in this subgroup
ranged between 0.5 and 7.2 Joules. Secondary outcome measures of
painfree grip strength, pain pressure threshold, sick leave and
follow-up data from 3 to 8 weeks after the end of treatment,
showed consistently significant results in favour of the same LLLT
subgroup (p < 0.02). No serious side-effects were reported.
CONCLUSION: LLLT
administered with optimal doses of 904 nm and possibly 632 nm
wavelengths directly to the lateral elbow tendon insertions, seem
to offer short-term pain relief and less disability in LET,
both alone and in conjunction with an exercise regimen. This
finding contradicts the conclusions of previous reviews which
failed to assess treatment procedures, wavelengths and optimal
doses.
TMJ
Effectiveness of low-level laser therapy in
temporomandibular joint disorders: a placebo-controlled study
Fikácková H, Dostálová T, Navrátil L, Klaschka J.
Institute of Biophysics and Informatics, 1st Medical Faculty,
Charles University, Prague, Czech Republic.
Photomed Laser Surg. 2007 Aug;25(4):297-303. [PMID:
17803388]
OBJECTIVE: Low-level laser therapy (LLLT)
treatment for pain caused by temporomandibular joint disorders (TMD)
was investigated in a controlled study comparing applied energy
density, subgroups of TMD, and duration
of disorders.
BACKGROUND DATA:
Although LLLT is a physical therapy used
in the treatment of musculoskeletal disorders, there is little
evidence for its effectiveness in the treatment of TMD.
METHODS: The study group of 61 patients
was treated with 10 J/cm(2) or 15 J/cm(2), and the control group
of 19 patients was treated with 0.1 J/cm(2). LLLT
was performed by a GaAlAs diode laser with output of 400 mW
emitting radiation wavelength of 830 nm in 10 sessions. The probe
with aperture 0.2 cm(2) was placed over the painful muscle spots
in the patients with myofascial pain. In patients with TMD
arthralgia the probe was placed behind, in front of, and above the
mandibular condyle, and into the meatus acusticus externus.
Changes in pain were evaluated by self-administered questionnaire.
RESULTS: Application of 10 J/cm(2) or 15
J/cm(2) was significantly more effective in reducing pain compared
to placebo, but there were no significant differences between the
energy densities used in the study group and between patients with
myofascial pain and temporomandibular joint arthralgia. Results
were marked in those with chronic pain. CONCLUSION:
The results suggest that LLLT
(application of 10 J/cm(2) and 15 J/cm(2)) can be considered as a
useful method for the treatment of TMD-related
pain, especially long lasting pain.
Arthralgia of the temporomandibular joint and
low-level laser therapy
Fikácková H, Dostálová T, Vosická R, Peterová V, Navrátil
L, Lesák J.
Institute of Biophysics and Informatics, 1st Medical Faculty,
Charles University, Prague, Czech Republic. hfikackova@hotmail.com
Photomed Laser Surg. 2006 Aug;24(4):522-7. [PMID:
16942435]
OBJECTIVE: This case report describes
the treatment of a patient with arthralgia of the
temporomandibular joint (TMJ) caused by
disc displacement.
BACKGROUND DATA:
The goal of the treatment of TMJ
arthralgia is to decrease pain by promotion of the musculoskeletal
system’s natural healing ability.
METHODS: This report describes the
complex treatment of TMJ arthralgia.
Low-level laser therapy (LLLT) was
chosen for its antiinflammatory and analgesic effects. Laser
therapy was carried out using the GaAlAs diode laser with an
output power of 400 mW, emitting radiation with a wavelength of
830 nm, and having energy density of 15 J/cm2; the laser radiation
was applied by contact mode on four targeted spots in 10 sessions.
Physiotherapy was recommended to this patient to prevent the
injury of intraarticular tissue caused by incorrect movement
during opening of the mouth. Splint stabilization and prosthetic
treatment were used to reduce overloading of the TMJ,
resulting from unstable occlusion and to help repositioning of the
dislocated disc.
RESULTS: Five applications of LLLT
led to decrease of pain in the area of the TMJ
on the Visual Analog Scale, from 20 to 5 mm. The anti-inflammatory
effect of the laser was confirmed by thermographic examination.
Before treatment, the temperature differences between the areas of
the normal TMJ and TMJ
with arthralgia was higher than 0.5 degrees C. However, at the
conclusion of LLLT, temperatures in the
areas surrounding the TMJ were
equalized. CONCLUSION: This study showed
the effectiveness of complex non-invasive treatment in patients
with arthralgia of the TMJ. The
analgesic and anti-inflammatory effects of LLLT
were confirmed by infrared thermography.
Wound healing
Effect of low-level laser therapy on inflammatory
reactions during wound healing: comparison with meloxicam
Viegas VN, Abreu ME, Viezzer C, Machado DC, Filho MS, Silva DN,
Pagnoncelli RM.
School of Dentistry, Laser Center, Pontifícia Universidade
Católica do Rio Grande do Sul (PUCRS),
Porto Alegre, RS, Brazil.
Photomed Laser Surg. 2007 Dec;25(6):467-73. [PMID:
18158747]
OBJECTIVE: This study evaluated the
action of low-level laser therapy (LLLT)
on the modulation of inflammatory reactions during wound healing
in comparison with meloxicam. BACKGROUND
DATA: LLLT has
been recommended for the postoperative period because of its
ability to speed healing of wounds. However, data in the
literature are in disagreement about its anti-inflammatory action.
METHODS: Standardized circular wounds
were made on the backs of 64 Wistar rats. The animals were divided
into four groups according to the selected postoperative therapy:
group A-control; group B-administration of meloxicam; and groups C
and D-irradiation with red (lambda = 685 nm) and infrared (lambda
= 830 nm) laser energy, respectively. The animals were killed at
12, 36, and 72 h and 7 days after the procedure.
RESULTS: Microscopic analysis revealed
significant vascular activation of irradiated sites in the first
36 h. Only group B showed decreases in the intensity of
polymorphonuclear infiltrates and edema. Group D showed a higher
degree of organization and maturation of collagen fibers than the
other groups at 72 h. The animals in group C showed the best
healing pattern at 7 days. The anti-inflammatory action of
meloxicam was confirmed by the results obtained in this research.
The quantification of interleukin-1beta (IL-1beta) mRNA by
real-time polymerase chain reaction (PCR)
did not show any reduction in the inflammatory process in the
irradiated groups when compared to the other groups.
CONCLUSIONS: LLLT
improves the quality of histologic repair and is useful during
wound healing. However, with the methods used in this study the
laser energy did not minimize tissue inflammatory reactions.
Low-Level Laser Therapy Facilitates Superficial
Wound Healing in Humans: A Triple-Blind, Sham-Controlled Study
Hopkins JT, McLoda TA, Seegmiller JG, David Baxter G.
Brigham Young University, Provo, UT.
J Athl Train. 2004 Sep;39(3):223-229. [PMID:
15496990]
OBJECTIVE: Low-level laser therapy (LLLT)
has been promoted for its beneficial effects on tissue healing and
pain relief. However, according to the results of in vivo studies,
the effectiveness of this modality varies. Our purpose was to
assess the putative effects of LLLT on
healing using an experimental wound model. DESIGN
AND SETTING:
We used a randomized, triple-blind, placebo-controlled design with
2 within-subjects factors (wound and time) and 1 between-subjects
factor (group). Data were collected in the laboratory setting. SUBJECTS:
Twenty-two healthy subjects (age = 21 +/- 1 years, height = 175.6
+/- 9.8 cm, mass = 76.2 +/- 14.2 kg). MEASUREMENTS:
Two standardized 1.27-cm(2) abrasions were induced on the anterior
forearm. After wound cleaning, standardized digital photos were
recorded. Each subject then received LLLT
(8 J/cm(2); treatment time = 2 minutes, 5 seconds; pulse rate =
700 Hz) to 1 of the 2 randomly chosen wounds from either a laser
or a sham 46-diode cluster head. Subjects reported back to the
laboratory on days 2 to 10 to be photographed and receive LLLT
and on day 20 to be photographed. Data were analyzed for wound
contraction (area), color changes (chromatic red), and luminance.
RESULTS: A group x wound x time
interaction was detected for area measurements. At days 6, 8, and
10, follow-up testing revealed that the laser group had smaller
wounds than the sham group for both the treated and the untreated
wounds (P < .05). No group x wound x time differences were
detected for chromatic red or luminance.
CONCLUSIONS: The LLLT
resulted in enhanced healing as measured by wound contraction. The
untreated wounds in subjects treated with LLLT
contracted more than the wounds in the sham group, so LLLT
may produce an indirect healing effect on surrounding tissues.
These data indicate that LLLT is an
effective modality to facilitate wound contraction of
partial-thickness wounds.
Dose and wavelength of laser light have influence
on the repair of cutaneous wounds
Mendez TM, Pinheiro AL, Pacheco MT, Nascimento PM, Ramalho LM.
IP&D, Univap & School of Dentistry, Universidade do
Vale do Paraíba, São José dos Campos, São Paulo, Brazil.
J Clin Laser Med Surg. 2004 Feb;22(1):19-25. [PMID:
15117483]
OBJECTIVE: The objective of the
present study was to compare histologically the effect of GaAlAs
(lambda 830 nm, phi approximately 2 mm(2), 35 mW) and InGaAlP
(lambda 685 nm, phi approximately 2 mm(2), 35 mW) lasers, alone or
in association with doses of 20 or 50 J/cm(2) on cutaneous wounds
in the dorsum of the Wistar rat. Background Data: The healing time
of surgical wounds is of extreme importance and it is usually
associated with a post-operative period free of infection and with
less pain and inflammation.
MATERIALS AND METHODS:
Sixty Wistar rats were divided into seven groups: Group I –
control (non-irradiated); Group II – lambda 685 nm, 20 J/cm(2);
Group III – lambda 830 nm, 20 J/cm(2);
Group IV – lambda 685 nm and lambda 830 nm, 20 J/cm(2); Group V
– lambda 685 nm, 50 J/cm(2)); Group VI – lambda 830 nm, 50
J/cm(2); and Group VII – lambda 685 nm
and 830 nm, 50 J/cm(2). The animals were sacrificed 3, 5, and 7
days after surgery.
RESULTS: Light microscopic analysis
using H&E and Picrosírius stains showed that, at the end of
the experimental period, irradiated subjects showed increased
collagen production and organization when compared to
non-irradiated controls. Inflammation was still present in all
groups at this time.
CONCLUSION: Group IV (lambda 830 nm and
lambda 685 nm, 20 J/cm(2)) presented better results at the end of
the experimental period. It is concluded that low-level light
therapy (LLLT) can have a positive
biomodulatory effect on the repair of cutaneous wounds.
Wound healing of animal and human body sport and
traffic accident injuries using low-level therapy treatment; a
randomized clinical study of seventy-four patients with control
group
Simunovic Z, Ivankovich AD, Depolo A.
Journal of Clinical Laser Medicine and Surgery (2000)
Apr;18(2):67-73
The main objective was to assess the efficacy of low level
laser therapy (LLLT) on wound healing in
rabbits and humans. The initial research was a randomized
controlled animal study, to evaluate the effects of laser
irradiation on the healing of surgical wounds in rabbits. The
application of LLLT on the human body is
analogous to those of similar physiologic structure in animal
tissue. This study was continued on humans, 74 patients with
injuries to the following anatomic locations: ankle and knee,
bilaterally, Achilles tendon; epicondylitis; shoulder; wrist;
interphalangeal joints of hands, unilaterally. All patients has
surgery prior to LLLT. Two laser devices
were used: infrared diode laser (GaAIAs) 830 nm continuous wave
for treatment of trigger points (TPs) and HeNe 632.8 nm combined
with diode laser 904 nm pulsed wave for scanning procedure. Both
were applied as monotherapy during the study. Results were
observed and measured according to these clinical parameters:
redness, heat, pain, swelling and loss of function, and finally
submitted to statistical analysis via chi2 test. Results: After
comparing the healing process between two groups of patients, the
following results were noted: wound healing was significantly
accelerated (25%-35%) in the patients treated with LLLT.
Pain relief and functional recovery of those treated with LLLT
were significantly improved compared to untreated patients. In
addition to accelerated wound healing, LLLT
for postoperative sport-and traffic-related injuries avoids side
effects of drugs, accelerates functional recovery, allows earlier
return to work, training and sport competition.
Laser and Sports Medicine in Plastic and
Reconstructive Surgery
Junichiro Kubota M.D.
Department of Plastic and Reconstructive Surgery, Kyorin
University School of Medicine, Tokyo, Japan.
Flap survival with diode laser therapy: Skin flap or graft
surgery are major procedures in plastic and reconstructive
surgery. Skin flap necrosis has been a problem. The author
reported on the enhanced blood flow following the low reactive
laser therapy in skin flaps. The 830 nm diode laser (20 – 60 mw)
irradiated flaps showed a greater perfusion, a greater number of
blood vessels, and a higher rate of survival areas than the
control flaps in the rat models and clinical cases. Improvement of
wound healing with diode laser therapy: Diode laser therapy was
indicated for traumatic skin ulcers from sport activities and
traffic accidents which were resistant to conservative treatment.
The diode laser system with a wavelength of 830 nm. and output
power of 150or 1000mw in continuous wave was applied with the
non-contact method to the area on the wound for one minute once a
day every day during the treatment period. The diode laser was
used successfully for the rapid enhanced healing of traumatic skin
ulcers.
Discussion: Most injured patients hope to avoid a surgical
operation, trying instead conservative treatments. The diode laser
therapy improved the flap circulation and wound healing of severe
skin ulcers. This therapy has been applied for temporomandibular
joint pain and favorable results were obtained. The diode laser
therapy proved to be particularly effective for pain attenuation.
The diode laser therapy offers an additional convenient, safe, and
side-effect free method. On the other hand, the Q-switched Nd:YAG
laser system consistently achieved good results concomitant with
easy and safe operation, with lightening of the target lesions.